
Key Indicators of Health Services
Describe about the Report for Singapore Healthcare System of Long-Term Care Policy.
Singapore health care system is extraordinary both regarding high quality and in cost control. The expenditure of health care is lowest regarding per capita and percentage of Gross Domestic product when compared to other highly developed countries. The government of Singapore plays an integral part to improve the health facilities. Singapore follows a philosophy that "avoidance is better than treatment." Therefore, it ensures the affordability of health services within the public health system through schemes such as Medisave and Medishield. These are the system of compulsory savings, price control, and subsidies. There are several nursing homes and public hospitals that work on grants through the charity organization. The growing cost is, however, the major concern in present health care system of Singapore. It is due to inflation and increases in the cost of medical devices and products.
The report will discuss about the key indicators of health services in Singapore. Further, it will discuss about the quality improvement of these health services along with its accessibility and enhancing affordability. The report will detail the primary health services available in Singapore and explain the health coverage system through its financing twin philosophies. Lastly, it will analyze its funding system. A thorough literature review will be performed to support the discussion.
In 2002, the OECD has initiated “Health Care Quality Indicators project”, with the aim to compare the health service quality in different countries. Based on the set of quality indicators one can identify the factors influencing the quality of health services (Pheng & Rui, 2016). Rotar et al., (2016) believes that these efforts will stimulate the policy makers and stakeholders cross-national learning. The crude birth and death rate in every 1000 population is 9.9 and 4.4 respectively. The total fertility rate/ female was found to be 1.3 and the under five mortality rate is 3. The primary cause of deaths includes cancer, pneumonia, cerebrovascular diseases and other chronic illness illustrated in the figure below. The total number of cancer patient discharged in the year 2009 and 2010 was 442 and 456 respectively. In the year 2011, the figure was 457 with negligible change (Rotar et al., 2016).


Accessibility, Raising Quality, and Enhancing Affordability
The government balances the individual responsibility and government control with the help of state control (Liu & Haseltine, 2016). The health care system of Singapore-
- Balances transparency
- Shares data with the market forces
- balances equity, expenditure, and choice with affordability
Accessibility, Raising Quality, and Enhancing Affordability
Singapore’s expectation from its health outcomes is evident from its "white paper Affordable Healthcare" released by the government of Singapore in 1993. This manifesto clearly embodies its vision, guiding philosophy, and a national health policy (Lim, 2016). Chin et al., (2016) reports that the rising quality of health care services is due to continued effort from Ministry of Health. It has implemented stringent legislations and enforced policies. It regulates the licensing of health centers under “Medical Clinics Act”. It conducts inspections and audits on a regularly basis. The Ministry of Health engages several professional bodies in regulating the professional through code of ethics and practice guidelines. It compares the performance of physicians and institutions annually through a management process. For this purpose, it utilizes “The National Health System Scorecard”. This Performance measurement, informs about areas of services that needs improvement. According to Goh et al., (2016), the “Health Sciences Authority” monitors the process of manufacturing, import, export, advertisement of health related products such as medicines, medical devices, and cosmetic products. It ensures that it meets the quality and safety standards. Accessibility of services has improved by reaching every community with high and low income earning populations through various categories of health services at all levels. For example, the “Community Health Assist Scheme” subsidizes the services such for colorectal cancer, diabetes, cervical cancer and various dental procedures. The number of hospitals and polyclinics has increased significantly since last decade (Haseltine, 2013).
Singapore has enhanced the patient’s affordability and accessibility of health services through its mix financing system, which offers multiple tiers of protection (Nizar & Chagani, 2016). Singapore has introduced a system of “co-payment” where people do not pay the total charge (Wouters et al., 2016). Government pays a part of the total expenditure while patients through Medisave, Medifund and Medishield system pay a fraction of it. These are discussed in detail in the later section of this report. There are 30 private and public hospitals having 1100 beds. In 2011, Public hospitals were reported with four million outpatient visits of which two-third were subsidized (Pheng & Rui, 2016).
Singapore has 1200 private clinics, which offers primary care for the citizens. Singapore subsidizes the primary health care costs in polyclinics such as GP visits and dentist visits for low income earning Singaporeans (Liu & Haseltine, 2016). There are 18 public polyclinics with multi-doctor facility and provides subsidized pharmacy services, health screening, outpatient care and immunization. In 2012, Singapore has introduced “The Community Health Assist Scheme” which subsidizes low income earning Singaporeans to visit private clinics participating in the scheme to treat specific chronic illnesses and acute conditions (Chin et al., 2016).
List of the Primary healthcare services: Polyclinics and Private medical clinics
According to Pheng & Rui, (2016), Singapore provides outpatient specialist care in several medical specialists such as oral cancer, neurological disorders, cancer, skin and cardiovascular diseases. The “National Heart Centre” is popular for these services. Patients avail these services through various government subsidies. Singapore provides after hours care. It has 30 clinics that offer 24 hours emergency care and its details are published online. People can access ambulances via emergency hotline as well as house call medical services that are available 24 hours (Penkunas et al., 2016). Therefore, the services are only short ride away.
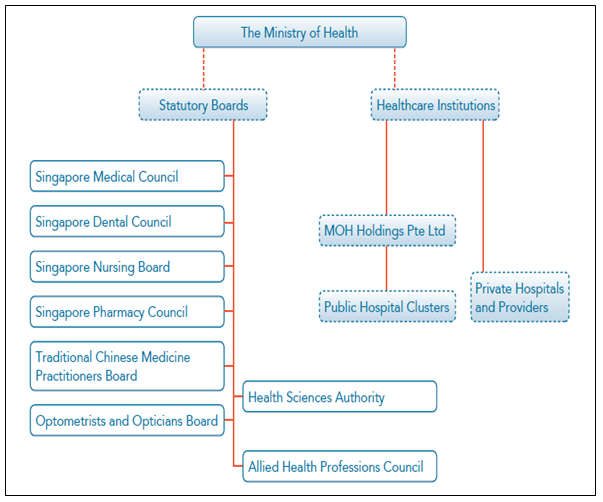
Figure: Structure of Singapore health system
(Source: Singapore Ministry of Health website)
Rotar et al., (2016), reported that there are regional hospitals in Singapore, which offers outpatient specialist services and acute inpatient care. They are equipped with emergency departments. There are 30 private and public hospitals having 1100 beds. In 2011, Public hospitals were reported with four million outpatient visits of which two-third were subsidized (Pheng & Rui, 2016). Singapore provides integrated mental health services through its “National Mental Health Blueprint” (Jesus et al., 2016). It has increased the accessibility of mental health services due to it rising demand. Since the last decade, there is increase in community-based services to treat mental illness such as dementia, eating disorders, addictions and others. The “Institute of Mental Health” provides acute tertiary care to the patients. It provides forensic services, rehabilitative care, counseling services for patients of all ages. The welfare organizations that provides residential care for patient include
- Singapore Association for Mental Health
- Singapore Anglican Community Services (Lim et al., 2016)
Singapore serves the needs of elder population by social support and long-term care through private operators and voluntary welfare centers. The government subsidizes these services for example Eldershield. It provides hospice care as well as home-based care (Rotar et al., 2016).
Singapore provides all its citizens with health care coverage based on its financing twin philosophies that are – individual responsibility and affordable health care (Haseltine, 2013). The country has improved the health care delivery system for its population, which enabled them to secure good health outcomes. It made it possible through –
Adopting latest technology
Mixed financing system
Market-based mechanism to promote competition (Malhotra et al., 2016)
Various international assessments have recognized these features. The country makes sure that all the citizens can access the primary health care. Singapore addresses the affordability issues through its mix financing system, which offers multiple tiers of protection (Nizar & Chagani, 2016). The government balances individual responsibility and government control with the help of -
Regional Hospitals
Government subsidies for primary health care
Individual savings accounts
hospital services and pharmaceuticals
Singapore has introduced a system of “co-payment” where people do not pay the total charge (Wouters et al., 2016). A part of the total expenditure is paid by government while a fraction of it is paid by patients through “Medisave and Medishield system”. Medisave is the health insurance plan, which allows the people to make substantial savings by accumulating funds (Liu & Haseltine, 2016). The citizens pay the fraction of health expenditure through Medisave. Singapore also has low cost insurance scheme called Medishield, for citizens who have low income and cannot meet the medical expenses. Receiving primary health care services in subsidized wards is useful. It secures the retirement of older workers as it offers increased rate of 1% for the first $60,000 of the total savings (Lim, 2016). Medifund is the service provided to those people who are unable to meet their assessed contribution. Eldershield is a policy which provides the citizens with insurance against expenses of private nursing homes. Additionally, Singapore has a system of Central Provident Fund (CPF). It is applicable for permanent residents and working citizens. This savings plan scheme is beneficial in accumulating the significant amount of fund through employers and employees. The members earn the higher rate of returns from their savings (Wouters et al., 2016). With the help of CPF, the country collects the pool of taxation revenue.
Singapore also provides privately financed health care services. The World Health Organization reports highlights that out of the total private expenditure on care, 10.1% was obtained from private prepaid plans (Wouters et al., 2016). High profit earning companies can avail this private insurance through integrated shield plans, which are Medisave-approved. People can receive additional benefits such as private and public hospitalizations and opt for Class A and B1 wards.
According to Chin et al., (2016), Ministry of Health (MOH) promotes competition and transparency by monitoring any variation in hospital costs in the country. It publishes “hospital bill sizes” and helps the hospitals to do more with less. Some of the improvements are decreased in LASIK prices by $1000/eye. MOH further encourages improvement by publishing health outcomes on its websites. This allows people to make informed choices.

Figure: Health coverage system in Singapore
(Source: www.moh.gov.sg)
According to Tan et al., (2010), the expenditure of health care in Singapore is lowest regarding per capita and percentage of Gross Domestic product (stable at 3%). The total expenditure of the government on the public health system constitutes 1.6% of annual GDP (Tan et al., 2010). However, the quality of care is not compromised and manages both the supply and demand sides of the market. Recently there is an added pressure on the health care system due to:
- lowering of infant mortality rate
- ageing
- Increasing life expectancy
Integrated Mental Health Services
These factors are responsible for increasing a cost of health services. To deal with it the government of Singapore is implementing case-mix (Liu & Haseltine, 2016). According to Wouters et al., (2016), case-mix can fund public hospitals for providing inpatient acute care. Case-mix implementation is based on hospital output. It ensures equity in financing healthcare. It enables data usage for quality improvement activities. Hospitals can receive information regarding their cost behavior. Hence, it will reinforce their drive for implementing cost-efficient health services (Liu & Haseltine, 2016). The case-mix information would help in rationalizing public hospitals’ fund. The funding will be proportional to resource use since there is a better definition of output. According to Rotar et al., (2016), MOH has announced that case-mix would only be used to fund acute inpatient and day surgery activity.

(Source : Rotar et al., 2016)
Conclusion
Singapore health stem is improving in terms of quality and affordability due to continued effort by the government. The country regulates both private and public health insurances. The Ministry of Health assesses the health care needs to plan and deliver them through range of hospitals and clinics. It finances policies, maintains adequate staffing and governs the public health system. This fast-paced world is increasing the pressure due to growing problems such stress related to family maintenance. The Singapore’s twin philosophies which anchor the financing system offers health coverage to all it citizens. Recently, there is an increase in a number of people falling sick without doctors being able to identify the reason. It is recommended that Singapore must develop strategies to determine the cause of non-health problems. It will help in reducing its extra expenditure and assist its growing population.
References
Chin, C. W. W., & Phua, K. H. (2016). Long-Term Care Policy: Singapore’s Experience. Journal of aging & social policy, 28(2), 113-129.
Goh, M. L., Ang, E. N., Chan, Y. H., He, H. G., & Vehviläinen-Julkunen, K. (2016). A descriptive quantitative study on multi-ethnic patient satisfaction with nursing care measured by the Revised Humane Caring Scale. Applied Nursing Research, 31, 126-131.
Haseltine, W. A. (2013). Affordable excellence: the Singapore healthcare story. Brookings Institution Press.
Jesus, T. S., Koh, G., Landry, M., Ong, P. H., Lopes, A. M., Green, P. L., & Hoenig, H. (2016). Finding the “Right Size” Physical Therapy Workforce: An International Perspective Across Four Countries. Physical therapy.
Lim, H. A., Tan, J. Y., Chua, J., Yoong, R. K., Lim, S. E., Kua, E. H., & Mahendran, R. (2016). Quality of life of family caregivers of cancer patients in Singapore and globally. Singapore medical journal.
Lim, J. (2016). Positivity and Overcoming “Under Happiness” in Singapore Healthcare. In Enabling Positive Attitudes and Experiences in Singapore (pp. 83-88).
Liu, C., & Haseltine, W. (2016). The Singaporean Health Care System, 2015.2015 International Profiles of Health Care Systems, 143.
Low, L. L., MMed, F. C. F. P., Tay, W. Y., & Ng, M. J. M. (2016). Frequent hospital admissions in Singapore: clinical risk factors and impact of socioeconomic status. Singapore medical journal.
Low, L. L., Wah, W., Ng, M. J., Tan, S. Y., Liu, N., & Lee, K. H. (2016). Housing as a social determinant of health in Singapore and its association with readmission risk and increased utilization of hospital services. Frontiers in Public Health, 4, 109.
Malhotra, C., Wong, G. C. S., Tan, B. C., Ng, C. S. H., Lee, N. C., Lau, C. S. L., ... & Finkelstein, E. A. (2016). Living with heart failure: Perspectives of patients from Singapore. Proceedings of Singapore Healthcare, 25(2), 92-97.
Nizar, H., & Chagani, P. (2016). Analysis of Health Care Delivery System in Pakistan and Singapore. International Journal of Nursing, 8(2).
Penkunas, M. J., Chan, A. W., Wong, C. H., de Korne, D. F., Tan, S. M., & Wong, S. F. (2016). The Role of a Multicomponent Home-Health Intervention in Reducing Caregiver Stress in Singapore: A Qualitative Study. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, gbw008.
Pheng, L. S., & Rui, Z. (2016). Facilities Management and Singapore’s Healthcare System. In Service Quality for Facilities Management in Hospitals (pp. 9-23). Springer Singapore.
Rotar, A. M., van den Berg, M. J., Kringos, D. S., & Klazinga, N. S. (2016). Reporting and use of the OECD Health Care Quality Indicators at national and regional level in 15 countries. International Journal for Quality in Health Care, mzw027.
Tan, W. S., Chong, W. F., Chua, K. S., Heng, B. H., & Chan, K. F. (2010). Factors associated with delayed discharges after inpatient stroke rehabilitation in Singapore. Annals Academy of Medicine Singapore, 39(6), 435.
Wouters, O. J., Cylus, J., Yang, W., Thomson, S., & McKee, M. (2016). Medical savings accounts: assessing their impact on efficiency, equity and financial protection in health care. Health Economics, Policy and Law,11(03), 321-335.
To export a reference to this article please select a referencing stye below:
My Assignment Help. (2017). Essay: Singapore Healthcare System. Retrieved from https://myassignmenthelp.com/free-samples/singapore-healthcare-system-long-term-care-policy.
"Essay: Singapore Healthcare System." My Assignment Help, 2017, https://myassignmenthelp.com/free-samples/singapore-healthcare-system-long-term-care-policy.
My Assignment Help (2017) Essay: Singapore Healthcare System [Online]. Available from: https://myassignmenthelp.com/free-samples/singapore-healthcare-system-long-term-care-policy
[Accessed 09 May 2025].
My Assignment Help. 'Essay: Singapore Healthcare System' (My Assignment Help, 2017) <https://myassignmenthelp.com/free-samples/singapore-healthcare-system-long-term-care-policy> accessed 09 May 2025.
My Assignment Help. Essay: Singapore Healthcare System [Internet]. My Assignment Help. 2017 [cited 09 May 2025]. Available from: https://myassignmenthelp.com/free-samples/singapore-healthcare-system-long-term-care-policy.